We’ll start outside and work through the low vision patient experience from the patient’s perspective. Dr. Long narrates and explains various details and expectations of the visit.
Every day we see patients who need the various glasses and devices described in the video, such as bioptics and bioptic telescopic glasses.
Low Vision Doctor Helping a Patient with Loss of Vision.
Take a look at the link to learn why your doctor should be referring you for low vision care. In 2018, the CEO of the American Academy of Ophthalmology declared that “referral for low vision rehabilitation is now the standard of care in ophthalmology.”
July 13, 2005 (I checked his chart), I remember examining my buddy, Dave, near the end of the day. He complained of blurred and distorted vision in one eye.
As doctors, through careful questioning, about 90% of the time we know, or think we know, what’s going on before we ever examine the patient. I knew my buddy had Idiopathic Central Serous Chorioretinopathy (ICSC). I had seen it before in another friend.
me: “Dave, I think I know what’s going on. Any extra stress in your life lately?”
Dave: “I’m not sure, not really…”
me: “Well anyway, I think I know what’s going on, but let’s get you dilated and take a look.”
Dave had active inflammation in one macula and suspicious lesions in the other. However, he did not have ICSC. The diagnosis was easy once I looked…he had Presumed Ocular Histoplasmosis Syndrome (POHS).
Dave’s story sticks in my mind because I was near tears when I gave him my diagnosis. I referred him to a retinal specialist and I knew that he would get laser treatment and would eventually be one of my low vision patients. But his case also sticks in my mind because there was something I didn’t know…
Rather than using a laser, the retinal specialist reported that he had injected a new cancer medication, Avastin, into Dave’s eye. Whaaat???!!! How would this help save his vision? Of course, now we know. His vision did improve and, despite eventually needing injections in both eyes, he still has good vision to this day. Amazing.
I believe there is a corollary here with low vision care:
There are new and unimaginable ways to help patients see better or even use other senses to complement poor vision. There are also often ways to acquire funding for expensive devices and to overcome other perceived obstacles.
If not me, seek another effective low vision provider via a Google search or other means. Low vision referral is the Standard of Care for good reason — there just might be some things that you didn’t know that you didn’t know.
Due to eye complications from juvenile rheumatoid arthritis, Sophie needed cataract surgery but was unable to have implants. The condition on not having a natural lens is called aphakia and it requires a patient to have strong glasses or contact lenses. Take a look at Sophie’s reaction to receiving new glasses with high-tech, super-modular lenses and her reaction to having comfortable soft contact lenses.
Hello, Dr. Long here sharing three low vision patient cases.
First we have Bobby who is partially-sighted secondary to trauma and ocular histoplasmosis and he is updating his bioptic driver’s licensure.
Second is De’Vante who has optic neuropathy and sees 20/120 with each eye. He wants to become a bioptic driver, be able to read, recognize faces, see fast food menus, and many other things.
Finally, Lonnie has diabetic retinopathy and neovascular glaucoma and I explain more about his condition and goals in the final segment of the video.
Here, in this two minute video, we feature three patients receiving their glasses and a tour of Dr. Long’s current office in Clarksville, Indiana.
The first gentlemen you see has seen Dr. Long for low vision care for many years now. He has not needed telescopic glasses until now and seems to be pretty excited about the help the bioptic style will afford him.
The second patient has fixed, dilated pupils and is extremely sensitive to light. Additionally, he is legally blind and needs both the tint and the magnification that comes with his prescription bioptic glasses and reading telescopic glasses.
Finally, the end of the video features a patient who was seen being evaluated in a previous video who is now picking up her Side Vision Awareness Glasses and being trained by our low vision technician, Casey.
See our patient’s reaction and learn more about the Side Vision Awareness Glasses
Since our last post about helping patients with one-sided peripheral vision loss due to stroke, Dr. Long has prescribed several pairs of Side Vision Awareness Glasses. Additionally, there is a new related product, the Full Field Side Vision Awareness Glasses system that Dr. Long has successfully prescribed now as well. Take a look at the video to learn about both!
Side Vision Awareness Glasses® (SVAG) were developed by Dr. Errol Rummel of Jackson, NJ, after years of treating people with stroke-related,or brain injury related hemianopsia (side vision loss).
Hemianopsia (loss of half the width of your field of vision) is one of the most common side effects of a stroke or traumatic brain injury. People can find themselves afraid to go out, disoriented, and struggling to make it through their day.
How the London Bridge would look to someone with a hemianopsia
Benefits of Side Vision Awareness Glasses (SVAG)
1. A wide viewing area, allowing better field awareness. And because SVAG have a vertical edge, a patient just needs to move their eyes a couple of millimeters to get into the SVAG area of the lens.
2. Cosmetically more attractive because the front of the lens is smooth, making the area with prism barely noticeable.
3. A higher index of refraction, so SVAG is a thinner, lighter, and more comfortable than other types of hemianopsia glasses.
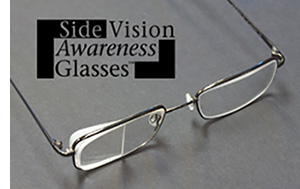
Notice the prism on the right lens of this pair of SVAG.
New Design Exclusive to Midwest Low Vision
Typically, these glasses have a prism on the back of the lens so that someone can use it when they need to by shifting their eyes to the left or the right. However, Dr. Rummel generously gifted Dr. Jarrod Long a set of his brand new full-field side vision awareness glasses. The work similarly to the standard SVAG but the entire lens is specially designed to shift the missing part of your vision into view. This expands a person’s awareness of objects in their path and enhances peripheral vision. Currently, Midwest Low Vision is one of the only practices in the Midwest with the full field SVAG.
New Full-Field SVAG design
This is a pair of the new full-field glasses. Notice how there is no extra attachment on either lens- instead, the entire lens is designed to adjust the field of view. You can see how the lens shifts the image of the eye chart to the left. This specific type of lens is ideal for someone missing their right visual field. The new design allows someone to see more of their side vision without compromising the view right in front of them.
Dr. Long is specially trained to prescribe and dispense the right pair of glasses for you or your loved ones. If this sounds like something that would improve your quality of life, please call for more information!
Our first Patriot Viewpoint dispensing and training.
As a low vision specialist, I like to find the simplest solutions to meet my patient’s goals. Sometimes it only takes a new, stronger pair of conventional glasses. Most of the time, however, it takes specialized telescopic, bioptic, microscopic, tinted, prismatic, and other styles of glasses.
Occasionally, none of these things work. More magnification than what optics will allow is needed. Enter “wearables” — magnification and vision enhancement technology that can be worn similarly to glasses. I have had the opportunity to try, and research, several of these emerging technological wonders. And trust me, there are many options out there with more being introduced regularly. They are all amazing!
It’s not new technology necessarily. It’s just that it has now become practical and realistically usable on a daily basis for multiple tasks on my patients’ “wish lists.” They are less cumbersome, more reliable, and more easily updated as software changes become available.
Casey, my head low vision technician, did all of the training today, but I was lucky enough to get the teary-eyed hug before he walked out the door. I have a feeling that won’t be the last hug from a patient whose vision is worse than 20/1000!