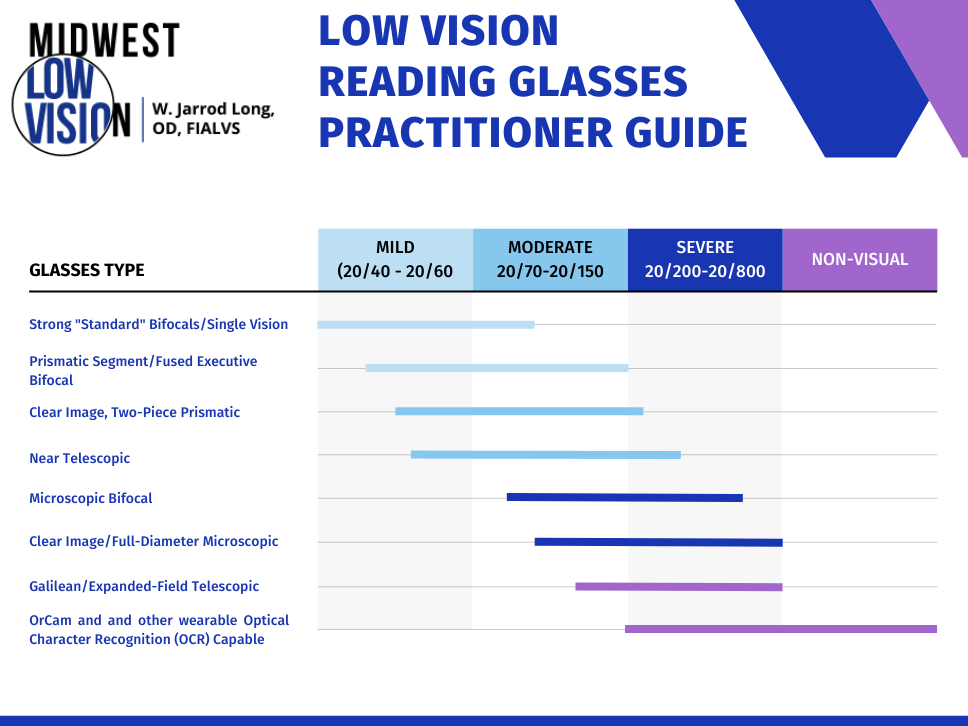
For patients with low vision, the loss of ability to read print can be challenging and disheartening, impacting work, household tasks, independence, and overall quality of life. Fortunately, there are specialized reading glasses that can support remaining vision and allow reading to be possible for these individuals once again. As low vision specialists or other eye care professionals, our task is to identify the type of low reading glasses that would best meet the patient’s needs. Read on to learn more about the most common categories of low vision glasses for reading.
Bifocal

The first option is simply strong standard bifocals or reading glasses. Often, simple prescription reading glasses with prisms incorporated and made by a local lab can work. You can also use a bifocal and perhaps decenter the segments a bit to create some base-in prism to aid convergence (eye teaming). The advantages of bifocals and prismatic reading glasses are:
- They are simpler in design.
- They are less expensive.
- They provide a wide field of view.
- They are binocular, allowing the use of both eyes together..
The main limitation of bifocals and stronger reading glasses is the working distance. The stronger the prescription, the closer the focal point needs to be, so there is a limit to the strength we can go with these low vision glasses.
Prismatic Segment Bifocal
Prismatic bifocals offer an alternative to decentering standard bifocals by incorporating a built-in, base-in prism into the glasses. These can have the D-shaped segment in the bottom, but with the appropriate base-in prism. This design provides the necessary prism for comfortable near vision without affecting distance vision, which is particularly beneficial in the higher powers.
Fused Executive Bifocal

Fused executive bifocal glasses consist of two lens segments fused together, one atop the other. They are called “executive” or “Franklin-style” because, like Ben Franklin’s original design, the lens goes all the way across the width of the frame. The design of these low vision glasses provides:
- The option for different strengths of prism in the top and bottom.
- A very large reading area at the bottom, and all the way across the lens.
The disadvantage of fused executive lenses is that they can be a little blurry at the lower edge of the lens; the distortion becomes greater with higher powers.
Clear-Image Microscopic and Prismatic

The Clear Image, two-piece microscopic and prismatic design, a system for a poorer vision level, provides greater edge-to-edge clarity. These lenses feature a two-piece design where the prism is offset in the magnifying lens, effectively reducing many distortions which normally occur with prisms and strong magnifying lenses.
The advantages of this design include:
- Clear edge-to-edge vision with a two-piece system.
- Extra prism support for higher powers.
The disadvantages of these lenses include:
- Cosmetic concerns due to the lens thickness.
- The need for a close working distance.
- Limited strength before prism thickness begins to restrict wearability.
I will use these when a patient needs, or just prefers, to have both eyes working together and doesn’t mind this close-up working distance. Looking from edge-to-edge in this lens it is extremely clear, and the binocularity is excellent.
Reading Telescopic

Reading telescopic glasses feature miniature telescopes to enhance near or immediate vision. The telescopes are mounted low and angled down to allow for comfortable close work. They can also be mounted on-center for computer use.
There are many different styles of near telescopic lenses. One model is the Ocutech SightScope NearView. Essentially, this is their distance system, but it includes prismatic caps that allow focus on near tasks. When distance vision is required, the caps can be flipped up and out of the way.
Another model is the Designs for Vision reading telescopic system. These lenses allow for an increased working distance compared to a microscope of a similar power, while still achieving an effective level of magnification.
In general, the advantages of the near telescopic glasses are:
- A defined working distance.
- Excellent edge-to-edge clarity.
- Availability of a binocular or monocular system.
Microscopic Bifocal

This system is very similar to a Clear Image, full-diameter microscope, but it’s smaller and can be built in as a bifocal. There are two different sizes: Type R is the larger size, and Type E is the smaller.
The advantages of these lenses are:
- As the microscope is incorporated into the bifocal, a patient can just wear these, and the microscope is always there, but out of the way when not in use.
- The lens offers high magnification with edge-to-edge clarity.
The disadvantage of the microscopic bifocal is a smaller field of view and the working distance must be very close.
Conclusion
There are a variety of low vision glasses to help people regain the ability to read and perform close-up tasks, and every option comes with unique advantages and disadvantages. The best choice depends on the patient’s needs and comfort with working distance and design. Careful selection of the appropriate lens can significantly improve a patient’s quality of life and independence. If you would like to learn more, get in touch with us today.